Does Eating Dates During Pregnancy Improve Labor? A review of the data. Plus, the blood sugar response to eating dates in various combos.

Read Lily’s article here: https://lilynicholsrdn.com/dates-pregnancy-labor/
Little known fact: Vitamin A is vital for breast health by Lily Nichols

Earlier this year, when I dove into the research on vitamin A to write this article on liver & organ meat, I rediscovered a paper on vitamin A and its role in breast health.
In my opinion, Vitamin A is one of the most misunderstood nutrients and something that I am constantly learning more about. Someday, maybe I’ll put together a webinar on the topic, but until then, I’ll share little snippets here, on my blog, and on social media.
With regards to breast health, our breasts depend on vitamin A to develop and function appropriately. This starts in utero, continues in childhood, dramatically shifts in puberty, again during pregnancy, lactation, weaning, and again during menopause.
Or, in fancy research terms: “retinoid signaling regulates almost all developmental stages of the mammary tissue.”
To highlight a few interesting points from this review article:
Hormones of lactation upregulate a number of pathways in vitamin A metabolism, which redirects vitamin A from fat stores and the liver to mammary tissue. Vitamin A is essential to the physical changes to breasts that facilitate adequate milk production as well as ensuring sufficient amounts of vitamin A are transferred into the milk.
You need ~60% MORE vitamin A during breastfeeding compared to pregnancy, even by conventional standards. To quote the article: “During the breastfeeding period, lactating mothers are susceptible to vitamin deficiency as the neonate feeds on her stores through the milk. Vitamin A is one of the most critical micronutrients in this period, affecting lung function and maturation, and thus susceptibility to infection. Inadequate maternal intake of vitamin A translates to an inadequate supply to the fetus during pregnancy and to the neonate during lactation through breast milk.”
In addition, a baby receives 60-fold more vitamin A during the first 6 months of life than they did during the entire 9 months of gestation. Vitamin A transfer in utero is carefully regulated, so early infancy is time where vitamin A stores are built up via vitamin A-rich breast milk. Unfortunately, many mothers are deficient in vitamin A and as a result, vitamin A levels in breast milk are also low. This is a very sensitive topic, but one I cover in excruciating detail in my Nutrition for Breastfeeding webinar — it’s 90 minutes devoted to the topic of nutrient transfer into breast milk.During weaning, the breasts go through a remodeling process called involution. Your breasts literally break down tissues that are no longer required (since you’re not producing milk anymore) and gradually rebuilds the breasts. Vitamin A is essential to this process. Interestingly (this is my anecdotal experience), I craved more vitamin A-rich foods, especially liver, during the first month postpartum and again during weaning. Coincidence? Or by design? Who knows…
There's probably a reason that liver was prized in ancestral cultures for fertility, pregnancy, and breastfeeding. I’d wager the vitamin A content is a big reason for that.
The Winners of Birth Become You's 2020 Image Celebration | Best of Birth Photography
Click on this link to see all of the incredible photos.
“Peace be Still” by Kathryn J Birth Stories in Dallas/Fort Worth, Texas



Headaches in Pregnancy: Is Tylenol Safe?
https://avivaromm.com/headaches-in-pregnancy/
Acetaminophen (Tylenol). Most people reach for it for everyday headaches like it’s no big deal, and 2/3 of women have used it in pregnancy. Yet acetaminophen is not benign. For example, it is one of the major contributors to liver disease in the US each year. Acetaminophen has also long been considered generally safe for use during all stages of pregnancy, making it the first-choice pain and fever medication for pregnant women. Given the large number of pregnant women using the drug, even a small increase in risk of adverse outcomes in offspring can have important implications for public health.
Tylenol started coming under scrutiny over its safety in pregnancy around 2014. Animal studies suggest that its use in pregnancy can have important implications for endocrine function, which is also important for neurodevelopment as well as normal sexual differentiation.
It’s also now been found, in three significant studies, to impact the developing human nervous system. In a major study of over 64,000 Danish mothers, maternal use during pregnancy was associated with as much as a 37% increase in hyperkinetic disorder, a severe form of ADHD, and a 30% increase in ADHD in their children. Risks of ADHD in children went up to 50% in women who took Tylenol for 20 weeks or more during pregnancy. Stronger associations were observed with use in more than one trimester during pregnancy, and the higher the frequency of use, the higher the risk of ADHD and hyperkinetic disorder.
A second more recent large study, of 7796 pregnant women who used acetaminophen at 18 and 32 weeks of pregnancy, again published in JAMA Pediatrics has confirmed these findings. This study found that children exposed to acetaminophen prenatally are at increased risk of multiple behavioral difficulties, and the associations do not appear to be explained by other behavioral or social factors.
Now a new study seems to confirm the concerns that acetaminophen, which can cross the placenta, does have fetal neurologic effects, and may be implicated in autism. Researchers analyzed umbilical cord blood from 996 births gathered as part of a study called the Boston Birth Cohort, a long-term study examining factors affecting pregnancy and child development. By the time the children were an average of 8.9 years, 25.8% had been diagnosed with ADHD, 6.6% with ASD and 4.2% with both ADHD and ASD. These rates corresponded to levels of prenatal acetaminophen exposure, compared to the lowest third of exposure, the middle third was associated with about 2.26 times the risk for ADHD, the highest third 2.86 times the risk., and for ASD risk the middle third had 2.14 times the risk, and nearly 4 times the risk for the highest third.
It is no surprise that Tylenol could be at the root of problems in developing babies – it depletes a chemical called glutathione that we rely on in our bodies for detoxification, and it also acts as a hormone disruptor. This study, published in JAMA Pediatrics, suggests that acetaminophen may influence fetal brain development.
This is also not the first time lack of acetaminophen safety in pregnancy has been raised – it has been linked to undescended testicles in males, an increased risk factor for infertility and later development of testicular cancer.
While it is unlikely that using acetaminophen a few times over the course of a pregnancy is likely to cause a problem, and the benefits outweigh risk for fever reduction in pregnancy, these studies are a reminder that medications should not be used unquestioningly during pregnancy. As one of the study researchers warned, “We should continually remain vigilant to the need to reappraise the evidence concerning the risk-benefit balances of medications in light of new research findings.”
So What’s a Mom to Do?
Headaches are a common prenatal problem, and acetaminophen has been considered safe to use, whereas other commonly used headache medications including ibuprofen and aspirin are not safe for use in pregnancy. So what can you do?
First, if you’ve taken Tylenol or another form of acetaminophen, don’t beat yourself up. The chances are, statistically speaking, still low that this will have any impact on your baby. And for fever and significant pain, it’s still considered the safest prenatal option. But we can’t just assumed it’s safe and it can have an impact, so the goal is to avoid it when you can and keep your duration of use as brief as possible.
Here are 5 safe, natural tips to help reduce headaches in pregnancy:
1. Apply a few drops of lavender oil, peppermint oil, or Tiger Balm to the temples; these have been shown to safely and effectively reduce headaches.
2. Many headaches are a result of neck and shoulder tension, so don’t overlook the value of massage, a gentle osteopathic manipulation, or craniosacral therapy for headache prevention and relief.
3. Magnesium can help reduce a tension headache; take 400 – 800 mg/day of magnesium glycinate, or if constipation is also a problem, magnesium citrate in the same dosage.
4. Take 2 ginger capsules once or twice daily if you feel a headache coming on; it is a natural anti-inflammatory herb that is considered safe in pregnancy
5. Take a hot bath with 2 cups of Epsom salts and 5-7 drops of lavender essential oil – the combination of magnesium in the Epsom salts, the aromatherapy from lavender, and hot water is deeply relaxing and can help relieve a headache.
Additionally, there are several herbs that are generally considered safe for use in pregnancy, including chamomile and lavender as teas or tinctures for mild headaches, and cramp bark (use tincture, 1/2 tsp. every 4 hours) and black cohosh (1/4 tsp. every 4 hours, NOT TO BE CONFUSED WITH BLUE COHOSH which is NOT TO BE USED in pregnancy) which I use in combination for more moderate headaches.
If you have a sudden onset of a headache, a more severe headache than usual, any visual changes or upper abdominal pain with your headache, or if you have a history of high blood pressure, please see your midwife or physician promptly as these can be signs of more serious illness, like pregnancy induced hypertension or preeclampsia.
If you have frequent headaches, getting to the root cause by making sure you are getting enough sleep, reducing excessive inflammation with dietary and lifestyle changes, making sure you are getting all of your nutrients, including essential fatty acids and protein, and looking into environmental allergies (sometimes a HEPA air filter can help!) is key to optimal wellness and the best thing you can do for you and baby. You might also want to consider working with a functional medicine, integrative medicine, or naturopathic physician skilled in pregnancy care.

I’m an Obstetrician. Giving Birth at Home Isn’t Irresponsible.
To improve access to safe birth at home, nationwide standards are necessary.

Dr. McLean is a board-certified obstetrician-gynecologist at the University of Washington in Seattle.
July 31, 2019
Jen Carnig holds her son, Wiley Lavoie, immediately after his birth at home in Brooklyn, N.Y., as her husband Dan Lavoie, daughter Olive and best friend Lisa Johnson look on.CreditCreditAlice Proujansky
Earlier this month, a Nebraska midwife, Angela Hock, was charged with negligent child abuse when a newborn died after complications from a breech birth at home. It’s worth noting that before this delivery, Ms. Hock, the proprietor of a business called Nebraska Birth Keeper, had performed 50 births at home without incident. Nonetheless, Ms. Hock was not certified to practice as a midwife.
It’s unfortunate that these are the stories about home birth that make headlines, because they give the practice a bad name, and contribute to a sense that home births are irresponsible, a danger to the mother and baby. Home births can be safe — as long as they occur within a system of standards and regulations of the very sort that were missing in Nebraska. When home birth is practiced in the shadows because of fear of recrimination, patients are worse off. We can change this by acknowledging that home birth is a reasonable medical choice, and by licensing midwives for home birth in all 50 states.
I have practiced as an obstetrician in Washington State since 2006. I attend births only in the hospital, but I frequently take care of patients who intended to give birth at home and ended up transferring to me when their labor didn’t progress normally. The American College of Obstetricians and Gynecologists (ACOG) had long opposed home birth, but in 2017 issued a committee opinion acknowledging that while “hospitals and accredited birth centers are the safest settings for birth, each woman has the right to make a medically informed decision about delivery.” By contrast, the Royal College of Obstetricians and Gynaecologists in the United Kingdom encourages home birth for women with uncomplicated pregnancies.
The source of this discrepancy, as well as a great deal of controversy, is that studies on newborn outcomes have come to conflicting conclusions. Data collected by researchers in California and Oregon suggest there may be an increased risk of death in babies born at home, while research in the Netherlands found no significant difference between the risks associated with planned home and planned hospital births. There is no high-quality data from randomized controlled trials because none have been conducted. This is in part because of ethical challenges and because very large numbers of patients would be needed to definitively detect differences.
What does seem clear, however, is that women undergo fewer interventions when delivering at home. A meta-analysis of more than 24,000 births in multiple countries found lower rates of severe laceration, episiotomy and cesarean section with planned home births compared to planned hospital births. Maternal outcomes are likely better at home because the possibility of unnecessary interventions is removed, although those interventions can still be obtained efficiently through transfer to a hospital. There is also evidence from Britain that there are fewer maternal complications, like postpartum hemorrhage, when women give birth at home. Cochrane, a trusted global network of health researchers, distilled these factors to what is most important: the overall safety of home birth is comparable to that of hospital birth for healthy patients assisted by experienced midwives.
Unfortunately, giving birth at a hospital isn’t universally safe. NPR reported that the United States is the only developed nation with an increasing rate of maternal death, which has more than doubledfrom 1987 to 2015. According to the Institute for Health Metrics and Evaluation, it is now nearly twice as dangerous to give birth here as it is in Britain, France or Germany, despite the fact that the United States spends more on health care per capita than these countries. ACOG notes that the statistics are even more dire among minorities, with black women being three to four times more likely to die than white women.
No one is immune to this risk. In 2017, Serena Williams almost died of a pulmonary embolism after delivering her daughter when her complaints of shortness of breath weren’t taken seriously at a Florida hospital. Researchers in Alabama and Georgia found that half of maternal deaths are caused by medically preventable complications like embolism, while the other half, including those linked to rising obesity rates and poor access to health care, cannot be blamed entirely on hospitals. Nevertheless, it remains understandable that pregnant women have started to lose trust in the medical establishment.
Marginalizing home birth only endangers patients. There is a better way to handle this, starting with formal accreditation. According to ACOG, approximately 35,000 births occur at home in the United States each year. State governments regulate the education and experience needed to qualify as a birth professional through licensure. Certified Professional Midwives are the only providers required to have training in home birth, but just 33 stateslicense CPMs to practice.
Nebraska is not one of those states — only Certified Nurse Midwives who also hold a nursing degree are licensed, and they are prohibited from attending births at home. This means that there are no birth professionals in Nebraska who are “properly certified” for home birth, making it difficult for patients who want a home birth to figure out who is qualified and how to access services.
A recent study published in PLOS One showed that in states where midwives are regulated and integrated into the health care system, rates of neonatal mortality, cesarean section and preterm birth are all lower, regardless of birth setting.
Washington State has the highest level of midwife integration in the country, and our group obstetric practice at the University of Washington’s Northwest Hospital routinely works hand in hand with community midwives to ensure patients are provided with the information and services they need.
The women of America deserve access to the best medical care possible. They deserve access to safe home birth, with a licensed midwife, in all states.

Probiotics lower GBS colonization levels
Lily Nichols highlights this very important research brief:
https://www.sciencedirect.com/science/article/pii/S1028455916300675
In one well-designed randomized trial, 99 pregnant women who tested positive for GBS at 35-37 weeks were given either a probiotic supplement or placebo. The probiotic supplement contained 10 billion CFU (each) or two strains of probiotic bacteria that have been specifically studied for their beneficial effects on vaginal health: Lactobacillus rhamnosus, GR-1® and Lactobacillus reuteri RC-14®.
The probiotic supplement was taken for an average of 20 days. At the time of admission to the hospital for delivery, a repeat screen for GBS was completed. Among the women who received probiotics, 43% tested negative for GBS compared to only 18% in the placebo group. Those are pretty compelling statistics, though note that it did not reverse colonization in all cases.
.
The study authors propose that supplementation w/ these strains be started in the third trimester.
QUESTIONS TO ASK YOUR CARE PROVIDER by Rachel Yellin
Questions to Ask your Care Provider
What is your philosophy on unmedicated births?
What do you think of women who want to give birth without any intervention?
What can you do/recommend to help me have as low intervention a birth a possible?
Do you practice in a group? Will I have a choice of practitioner? How many others do you share “call” with? What are the birth philosophies of the others on your team?
What percentage of your own patients births do you attend?
Will you be away for any period of time around my due date?
What are your routine procedures/interventions?
What percentage of your patients have unmedicated births? Epidural births? Cesarean births? Induced births? vacuum/forceps births? Episiotomy?
Are you willing to have a conversation with me about what I will need to support me in having a hypnosis-based birth?
Under what conditions do you recommend having an amniocentesis or ultrasound?
Do you tend to lean more towards “management of labor” or “mother directed birth”.
How much of my labor will you attend?
What is your view on doulas?
In the event that I need to give birth in an operating room, what will you do to support me in having my partner and doula in the operating and recovery room with me.
I may request that non-urgent medical providers be restricted. Do you support that?
What is your policy about fetal monitoring?
Under what circumstances is a fetal scalp electrode used?
What is your policy on my eating and drinking during labor?
Under what circumstances will you want to induce or augment my labor?
What percentage of your patients receive pitocin to stimulate labor?
What are your thoughts on artificial rupture of membranes?
If labor begins with spontaneous rupture of membranes, how long do you routinely wait before starting pitocin? What is the time limit in which you think my baby needs to be born?
When do you routinely suggest induction for reasons related to due dates?
I will want to give birth in my position of choice. Will you support that?
I will want to decline vaginal exams unless if I have a medical decision to make based on that information. Will you support that?
Will you support me in my decision about when to clamp the cord and when to cut the cord?
Will you support me in my desire to breastfeed my baby before any stitching is done.
How do you feel about me declining some of the newborn procedures?
Will you support me in delaying procedures?
What’s your opinion about circumcision?
How do you handle complications in labor such as “failure to progress.”
How do you handle breech birth? IF my baby were to be in a frank-breech position, would you support me in waiting until my labor starts and then having a cesarean?
Do you do VBACs?
If my baby needs to be born by cesarean, what is the policy about baby leaving the OR or staying with me and my partner in the OR?


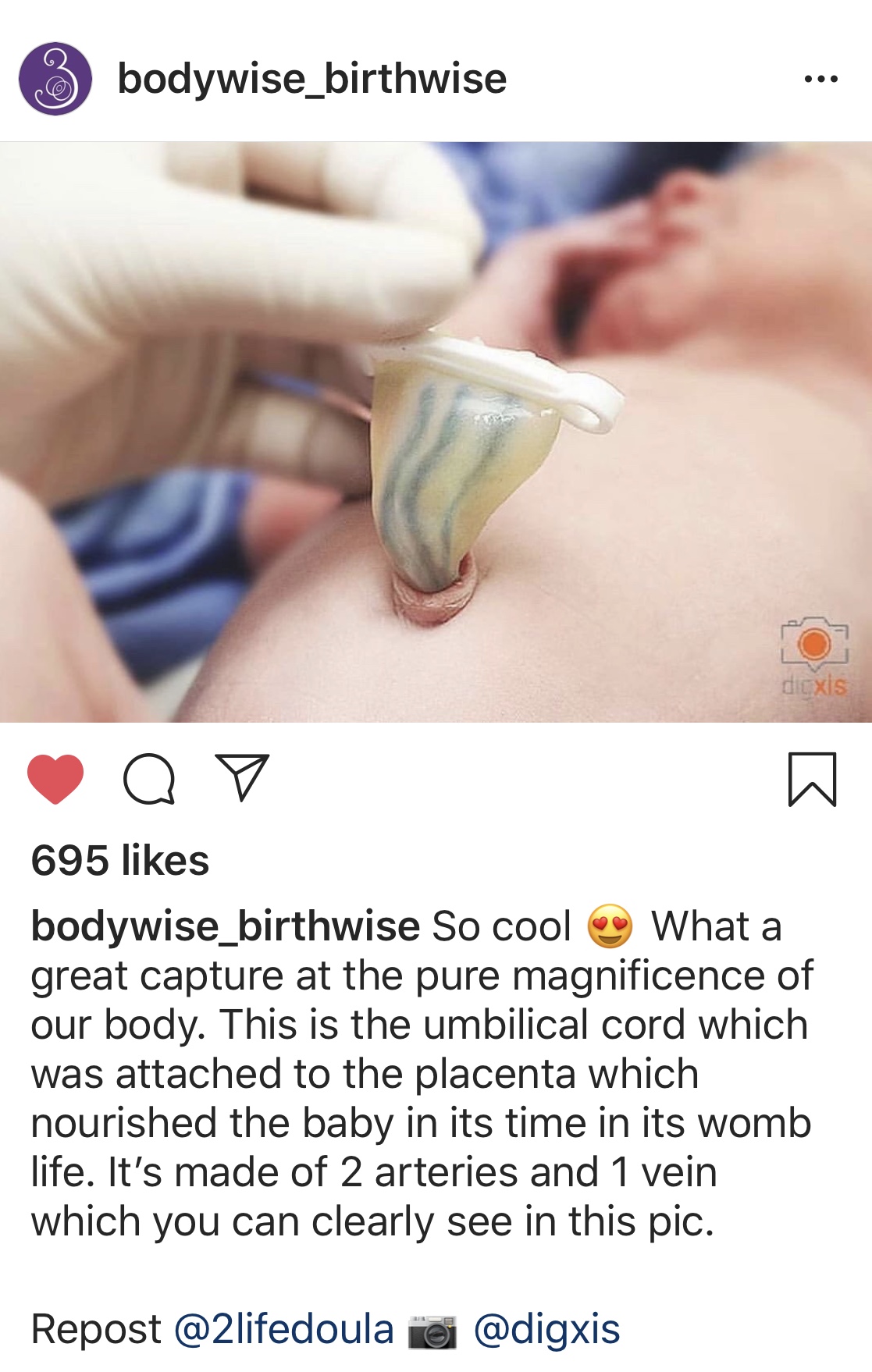
Placenta Encapsulation and Breastmilk supply
“Powdered Placenta Hominis was used for 57 cases of insufficient lactation. Within 4 days, 48 women had markedly increased milk production, with the remainder following suit over the next three days.” Bensky/Gamble. 1997. Materia Medica, Eastland Press, 549.

Hospital and Time of Delivery May Affect Mother’s HealthThe risk for complications in childbirth was highest during night shifts, weekends, holidays and in July.
Compared with daytime deliveries on weekdays, the risk for complications during night shifts was 21 percent higher, on weekends 9 percent higher and on holidays 29 percent higher.
The researchers also found an increased risk of 28 percent in teaching hospitals in July, when new residents begin their training. This difference was reduced to statistical insignificance by the following June.
https://www.nytimes.com/2019/03/04/well/family/hospital-pregnancy-childbirth-delivery-complications.html
Can your partner be your doula?
Partners know the birthing mom intimately. Doulas know birth intimately. Together we make a great team. Not sure if you need a doula?
Here's HBS’s handy checklist to explore if your partner is prepared to be your doula:
Has your partner attended births of people they aren't related to as a primary emotional, physical, and informational support person?
Does your partner regularly participate in continuing education opportunities on topics related to supporting families through pregnancy, birth, and the postpartum period?
Is your partner someone you'd consider a primary resource for information during pregnancy? What about after your baby is born?
Does your partner have referrals on hand in case you need extra support? Can they point you toward a great childbirth class, prenatal chiropractor, lactation counselor, pelvic floor physical therapist, prenatal massage therapist, ...?
Is your partner a member of any doula/birth professional groups or associations so they can learn from others' experience as well as their own?
Is your partner well-versed in the language of birth? Do they have a thorough grasp of commonly used medical terminology, abbreviations, acronyms and other language specific to labor?
Does your partner have an in-depth understanding of the ways medications and technology can be used during labor? Do they understand the common side effects of medications and procedures that are sometimes used in birth? And if so, are they practiced at communicating that information with people who are deep in labor to help them make thoughtful and informed decisions if the need arises?
Does your partner have a wide working knowledge of coping skills and comfort measures to help people through labor? Do they have tips and tricks up their sleeve that they can offer at pivotal moments during labor, based on their experience and knowledge?
Does your partner have advanced knowledge and skills to help identify ways you might be better supported during labor? Can they identify labor patterns that might indicate that a specific change in position for labor progress could be helpful?
If labor needs to be induced for whatever reason, can your partner walk you through what to expect from the induction process and what questions you might want to ask your care provider? What if a scheduled cesarean is necessary?
If there is a challenging situation during birth, does your partner have the experience and knowledge to offer a solution that may not have been offered by your care providers yet if the need arises?
Is your partner totally comfortable in a hospital labor and delivery room? Do they have tricks for helping YOU feel more comfortable there?
Does your partner have experience "holding space" for laboring parents? Are they practiced at staying balanced within themselves even in the uncomfortable, challenging, or even frightening moments that can happen during birth, all the while supporting you fully?
Does your partner have experience speaking to and touching people during birth? Are they in tune and responsive to the needs of someone who is in labor?
Is your partner used to spending hours upon hours in a small space with little nourishment and/or sleep while still supporting someone through their labor?
Thank you HB services for putting this checklist together! https://www.herobirthservices.com/blog/2018/9/19/long-beach-doula-your-partner-is-not-your-doula
The importance of Salt in Pregnancy
Ever wonder why so many pregnant women crave pickles and olives?
It’s probably the salt.
Salt gets a bad rap in conventional nutrition, but you need salt to survive.
When you’re pregnant, your body has more fluids on board (blood volume expands + amniotic fluid) and when you have more fluids, you need more salt to balance it out.
Think about it for a minute. If you’ve ever received IV fluids at the hospital, did they give you plain water? NO! They give you salt water because all of your bodily fluids also contain salt, where it serves as an electrolyte (among many other functions).
Many women are (erroneously) told to restrict salt as a means to avoid fluid retention or high blood pressure, but neither of these suggestions are scientifically sound.
A Cochrane review—a highly respected source of evidence-based analyses—concluded that advice to lower salt intake in pregnancy should NOT be recommended. This advice holds true even for women who have high blood pressure or preeclampsia (some research suggests that more salt, NOT LESS, is ideal in these situations).
In fact, restricting salt can have serious consequences, such as growth restriction in baby and even fetal loss.
As one study explains:
“Salt is one of the integral components for normal growth of fetuses. Salt restriction during pregnancy is connected to intrauterine growth restriction or death, low birth weight, organ underdevelopment and dysfunction in adulthood.” (Journal of Biomedical Science, 2016)
And another:
“Extra salt in the diet seems to be essential for the health of a pregnant woman, her fetus, placental development, and appropriate function.” (Journal of Reproductive Immunology, 2014)
I could go on and on about this, but I cover all the relevant research on this topic in Chapters 2 and 7 of my book, Real Food for Pregnancy.
The short answer is that salt is nothing to fear during pregnancy and, perhaps surprisingly, there are legitimate concerns about not getting ENOUGH salt.
So, salt your foods to taste and don’t ignore those salt cravings; your body is sending those signals for a reason.
Lily Nichols


Fascinating Facts
MATERNAL HEALTH FAST FACTS
(United States, 2016)
Live births: 3,945,875
Hospital births: 3,883,255 (98.4%)
CHARACTERISTICS OF LABOR
Epidural or spinal anesthesia during labor 2,901,486 (73.5%)
Induction of labor 967,811 (24.5%)
Augmentation of labor 826,783 (21.0%)
Steroids (glucocorticoids) for fetal lung maturation 93,931 (2.4%)
Antibiotics received by mother during labor 976,049 (24.7%)
Clinical chorioamnionitis during labor 60,505 (1.5%)
FINAL METHOD OF BIRTH
Vaginal, spontaneous 2,562,527 (65% of 3,945,875)
Vaginal, forceps 21,674 (0.5% of 3,945,875)
Vaginal, vacuum 100,602 (2.6% of 3,945,875)
Cesarean 1,258,581 (31.9% of 3,945,875)
Vaginal Birth After Cesarean 75,244 (12.4% of 601,788)
FETAL PRESENTATION
Cephalic (Head-down) 3,719,121 (94.8% of 3,945,875)
Breech 152,519 (3.9% of 3,945,875)
Other Fetal Presentation 51,444 (1.3% of 3,945,875)
https://www.cesareanrates.org/maternal-health-fast-facts/
LIstening to Mothers


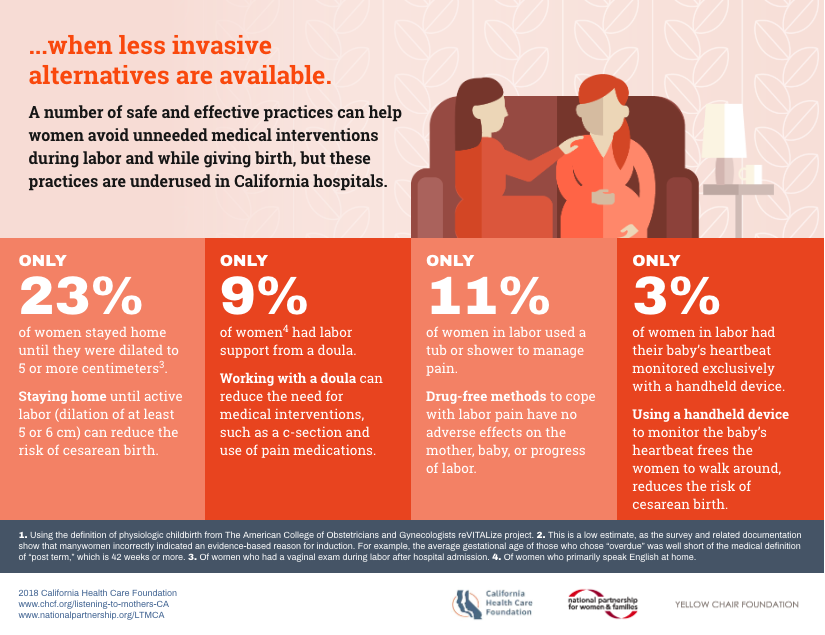
https://www.chcf.org/publication/infographic-overmedicalization-childbirth/